
Urethral Blockage From Prostate Cancer Treatment
What is a urethral stricture?
A urethral stricture is a narrowing of the urethra, which is the tube that carries urine from the bladder out of the body. This narrowing can occur anywhere along the length of the urethra, from the bladder to the external urethral opening.
What are the symptoms of a urethral stricture?
Symptoms of a urethral stricture may include a weakened or slow stream of urine, difficulty starting or stopping urination, frequent urination, pain or discomfort during urination, and urinary tract infections. In severe cases, a urethral stricture can cause complete blockage of the urethra, leading to urinary retention and other complications.
How can prostate cancer treatment lead to a urethral stricture?
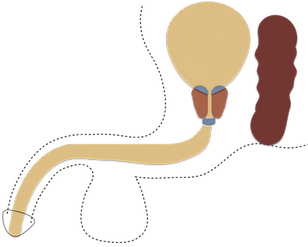
Prostate cancer treatment can cause a urethral stricture due to the location of the prostate gland and its close proximity to the urethra, which is the tube that carries urine out of the body. The urethra runs through the prostate gland in men (fig. 1), and treatments that target the prostate gland can potentially damage the urethra and cause a stricture. Common treatments for prostate cancer include surgery, radiation therapy, and brachytherapy. During surgery (radical prostatectomy), the prostate gland is completely removed, and the bladder neck is sewn to the urethra (see fig. 2). This connection (or anastomosis) is an area prone to narrowing or scarring. This occurs in about 5% of men undergoing radical prostatectomy. If the man also receives radiation after prostate surgery, then this connection is especially prone to stricture (the risk is over 10%).

bladder
prostate
back
bladder "neck"
sub-conscious sphincter
conscious sphincter
rectum
Figure 1.

bladder
rectum
front
back
urethra
prostate
Figure 2a.

rectum
bladder
urethra
Figure 2b.
Radiation therapy treats cancer by killing cancer cells. But, it can also cause damage to nearby non-cancerous tissue, like the urethra and bladder. Unlike surgery, urethral strictures from radiation can occur many years after the radiation has been given. This makes it harder to estimate the chance of a stricture, but it is probably less than 5%. Common places for a stricture to occur after radiation include the bladder neck, membranous urethra or bulbar urethra. Brachytherapy is radiation that is delivered in the form of radioactive seeds about the size of a grain of rice. These are implanted into the prostate. Like externally delivered radiation therapy, brachytherapy can cause damage to nearby non-cancerous tissues like the urethra. The chance of this happening is about 5%. This can be more likely if the seeds migrate out of the prostate and into the urethra. Men who receive brachytherapy AND external beam radiation are at especially elevated risk of urethral stricture, over 10%. Two x-rays of a man with a urethral stricture from brachytherapy are shown here. The first x-ray (fig. 3) shows the bladder as he tries to urinate. The dye in the bladder shows the blockage in the middle of the prostate, which is easily identifiable by all the radiation seeds in it. The second x-ray (fig. 4) shows the urethra as dye is squirted up through the tip of the penis. If you combine the two images you can see that he has a stricture that starts just below the prostate and extends to the mid-prostate.

Figure 3.

Figure 4.
How often does prostate cancer treatment lead to a urethral stricture?
Dr. Elliott received a grant from the American Cancer Society to study the impact of prostate cancer treatment on developing urinary problems later. He and his team used data from a national cancer registry (“SEER”) combined with billing records from Medicare to estimate the national incidence (or frequency) of these complications and how they were treated. The most common complication was urethral stricture. A graph (fig. 5) depicting the risk of urinary adverse events (meaning any urinary complication) with the different prostate cancer treatments is below. The way to interpret this graph is to see subtract out the background risk of these events – by this, we mean subtract out the frequency of developing urinary complications in men of a similar age, without prostate cancer. By subtracting out the background risk, you arrive at the attributable risk – the risk that can be attributed to (or blamed on) the prostate cancer treatment. Notice how, combination therapies increase the risk of complications, the most common of which is stricture.

RP = radical prostatectomy
BT = brachytherapy
EBRT = external beam radiation therapy
Control = similarly aged men without prostate cancer
Figure 5.
What treatment options are available for a urethral stricture caused by prostate cancer therapy?
The treatment options are similar to those for urethral strictures not caused by prostate cancer therapy. They include, dilation, urethrotomy or urethroplasty. The success rates with these treatments tend to be lower in men who have received radiation because radiation damages the blood vessels in the area, meaning that any treatment will have less blood flow to help it heal. Still, with careful treatment selection, we can often find a treatment that helps a man achieve success.
Dilation
A wire is passed through the stricture using a camera and then either a balloon or a series of metal dilators are used to stretch the urethra to normal size. Scar tissue is brittle, so it doesn’t really stretch; instead, it develops cracks (or fissures). It is especially brittle after radiation and less so after radical prostatectomy. The hope is that healthy urethra tissue will grow in to fill these cracks. Short strictures that have not received radiation and have not been treated before have a good chance of responding well to dilation – >50% of these men will still have an open urethra a year or two later. But men who have received radiation, with strictures longer than 2cm (about 1 inch) or men who have a stricture that has recurred after prior treatments, have a low success rate with dilation.
Urethrotomy
A scope (camera) with a small knife (about the size of a Q-tip) on the end of it is used to make a few cuts in the scar tissue. Like with dilation, the hope is that these cuts will fill in with normal urethral tissue as the site heals. Success rates are similar to dilation.
Self-dilation
One way to deal with the stricture without further surgery is to perform self-dilation at home. Once every other day, a person passes a catheter or inflatable balloon across the stricture to keep it open. By repeating this procedure frequently, you are encouraging the stricture to stay open, rather than re-dilating it from scratch every time. Therefore, this procedure is not as painful as you might imagine. Especially for men with radiation-induced strictures, self-dilation can offer a way to keep the stricture open without surgery. For those not interested in self-dilation, there are more invasive alternatives (see below).
Drug coated balloon
The Optilume drug-coated balloon is a new option. The procedure is performed just like a regular balloon dilation but is more successful. The balloon is coated with paclitaxel which is a chemotherapy drug that fights scar tissue reformation. Just a like a regular dilation, it creates cracks in the scar; the paclitaxel dissolves into the tissue in these cracks. The concept is that by delaying scar tissue formation, it allows more time for normal urethral tissue to grow instead. Dr. Elliott was the lead investigator for the study that led to the FDA approval of this device and is an expert on its use. In that study, 127 men were randomized to receive either the Optilume or a plain balloon or urethrotomy. Success rates at 1 year were 75% in the Optilume group compared to 27% in the control group. For a few weeks after the procedure, Optilume results in more burning with urination and more blood in the urine than dilation with a plain balloon. None of these men had previous prostatectomy and only a few had previous radiation. So, it is hard to extrapolate these results to the strictures after prostate cancer therapy. But, given these encouraging results, we are using Optilume in men with previous radiation and we are seeing better results than with plain balloon dilation. Optilume may not offer a permanent cure for radiation-induced strictures; but, if it can at least increase the interval of time before one needs another treatment then that is an improvement.
Urethroplasty
This is a plastic surgical reconstruction of the urethra, a procedure in which Dr. Elliott is an expert. There are many different ways to perform a urethroplasty, depending on the length and location of the stricture. But, essentially, through an incision about 4 inches long, a new urethral tube is constructed. If the stricture is short then we remove the stricture and sew the two healthy ends of the urethra together again. If the stricture is longer than 2 cm (about 1 inch) then we cannot remove the stricture and, instead, open the stricture and add to the circumference of the urethra in that area using a tissue graft from the inside of the cheek. The cheek tissue is very similar to the urethral tissue, so it performs very well. Success rates of urethroplasty are about 90% in non-radiated strictures and about 70% in radiated strictures.
Will treatment of a urethral stricture after prostate cancer therapy cause incontinence?
The most common cause of stress urinary incontinence in men is prostate cancer treatment. Either prostate removal (radical prostatectomy) or radiation treatment can damage the urethral sphincter. The sphincter is the valve that helps hold the urine inside the bladder. There are two sphincters in men. One sphincter is located at the top of the prostate, where it meets with the bladder (bladder neck) and is controlled subconsciously. The other sphincter is located at the bottom of the prostate, where it meets with the pelvic floor, and is controlled consciously. When you are cold or nervous and can’t pee, that is the subconscious sphincter that isn’t relaxing. When you try told hold back urination by tightening your muscles, that is the conscious sphincter working. The subconscious sphincter is removed in its entirety during a radical prostatectomy and a man becomes completely dependent on conscious tightening of the lower sphincter. But, the conscious sphincter can also be damaged during a radical prostatectomy. It wraps around the lowest part of the prostate and connects it to the pelvic floor. So, the conscious sphincter fibers must be carefully separated from the prostate during radical prostatectomy. Either due to an advanced cancer or an oddly shaped prostate or sphincter, it can be hard to save all the sphincter fibers. Like radical prostatectomy, radiation can also damage the sphincter muscles. Its effect, though, is more gradual. Surgery causes damage immediately and things usually improve slightly after surgery. Radiation causes damage over the long-term. Radiation kills the cancer cells but will also kill some of the nearby normal cells, like the sphincter muscles. So, someone can be continent of urine right after radiation and develop incontinence 5-10 years later. Men who undergo radical prostatectomy AND radiation combined are at particularly high risk for urinary incontinence. Men who have had enough damage to the urethra from radiation or prostate surgery to have a urethral stricture often also have damage to the conscious sphincter muscle. A man may not know just how much damage there is to the sphincter muscle when he has a stricture because the stricture can help with holding back the urine. In fact, it holds back the urine so well that men have difficulty urinating. But, once the stricture is treated and the urethra is open, the man will become completely dependent on his conscious sphincter to hold back the urine. Only then will he appreciate how incontinent he truly is. So, men can become more incontinent after treatment of a prostate cancer therapy-related urethral stricture. But, it is probably not the stricture treatment that caused the incontinence. It is the prostate cancer treatment that removed caused the incontinence. The stricture treatment just removed the blockage and unveiled the underlying incontinence.
bladder
prostate
back
bladder "neck"
sub-conscious sphincter
conscious sphincter
rectum